Community-driven Health Care Quality Improvement: a Blueprint to Reduce Perinatal Mortality in Ethiopia
story
Mestawot Mekonnen, a midwife in Dekebora Health Center of Lume Woreda.
In many parts of Ethiopia, health service utilization is hindered by a fundamental disconnect between local health facilities and the communities they serve. Through our Gates Foundation-funded Improve Primary Health Care Service Delivery project, JSI works closely with the Ministry of Health to tailor approaches that foster collaboration between health facilities and communities. Bridging the gap between community members and facility-based care leads to high-quality health care accessible to those who need it most.
The Combined Community Facility Quality Improvement (CCFQI) approach goes beyond community participation by bringing together health providers, community health workers, community and religious leaders, representatives of schools and women development groups, and local government officials, to identify, prioritize, and address major problems of maternal and child health. A given CCFQI committee can have up to 13 members who meet every month.
South Bench, in the South West Ethiopia Peoples’ Region, provides primary care to its population through a network of six health centers and 28 health posts. After developing a CCFQI implementation guide, an orientation on quality improvement was given by JSI to community groups and with health workers. Local government administrations and health facilities recruited health workers, legislative and religious leaders, and community members to form a CCFQI committee. The committee meets monthly to discuss and identify major health challenges in their locality.
One of the critical challenges identified in South Bench, by both community members and health workers alike, was the persistently high rate of perinatal deaths. Reports obtained from District Health Information Software substantiated the concern. Before the intervention, the intervention area experienced a high and unstable perinatal mortality rate, fluctuating between 124 and 86 deaths per 1,000 births, reflecting persistent challenges in the quality of maternal and newborn care.
In discussing this issue, the committee identified some contributing factors: late initiation of antenatal care appeared common among mothers, and almost half of all deliveries took place at home in unsafe and unhygienic conditions. These practices significantly increased the risk of preventable complications and delays in receiving appropriate care.
The committee prioritized activities at both the community and facility levels. Early identification of pregnant mothers and facilitating family conversations were among the prioritized actions pursued at community level; while strengthening the referral system, maternal and child health service delivery skills-building among health workers, clinical audits, and improving maternity waiting home infrastructure were identified as priority actions at facility level.
Each member of the CCFQI coordinating committee played a vital role in addressing the identified problem: Sister Gebremicheal, a village health leader, for instance, proactively identifies pregnant women and facilitates their connection with a health facility to initiate antenatal care (ANC). Concurrently, religious leaders like Mamo Zewde began educating church members about the importance of ANC attendance and skilled delivery.
JSI provided mobile ultrasound and solar panel power source to support service delivery at local health facilities, while also applying Network of Care – an approach used to further enhance effective facility and community communication, referral protocol adherence, and communication between public and private facilities.
Earlier and increased ANC attendance driven by community action, coupled with facility-level improvements in service delivery led to a reduction in perinatal mortality by 48% in South Bench Woreda.
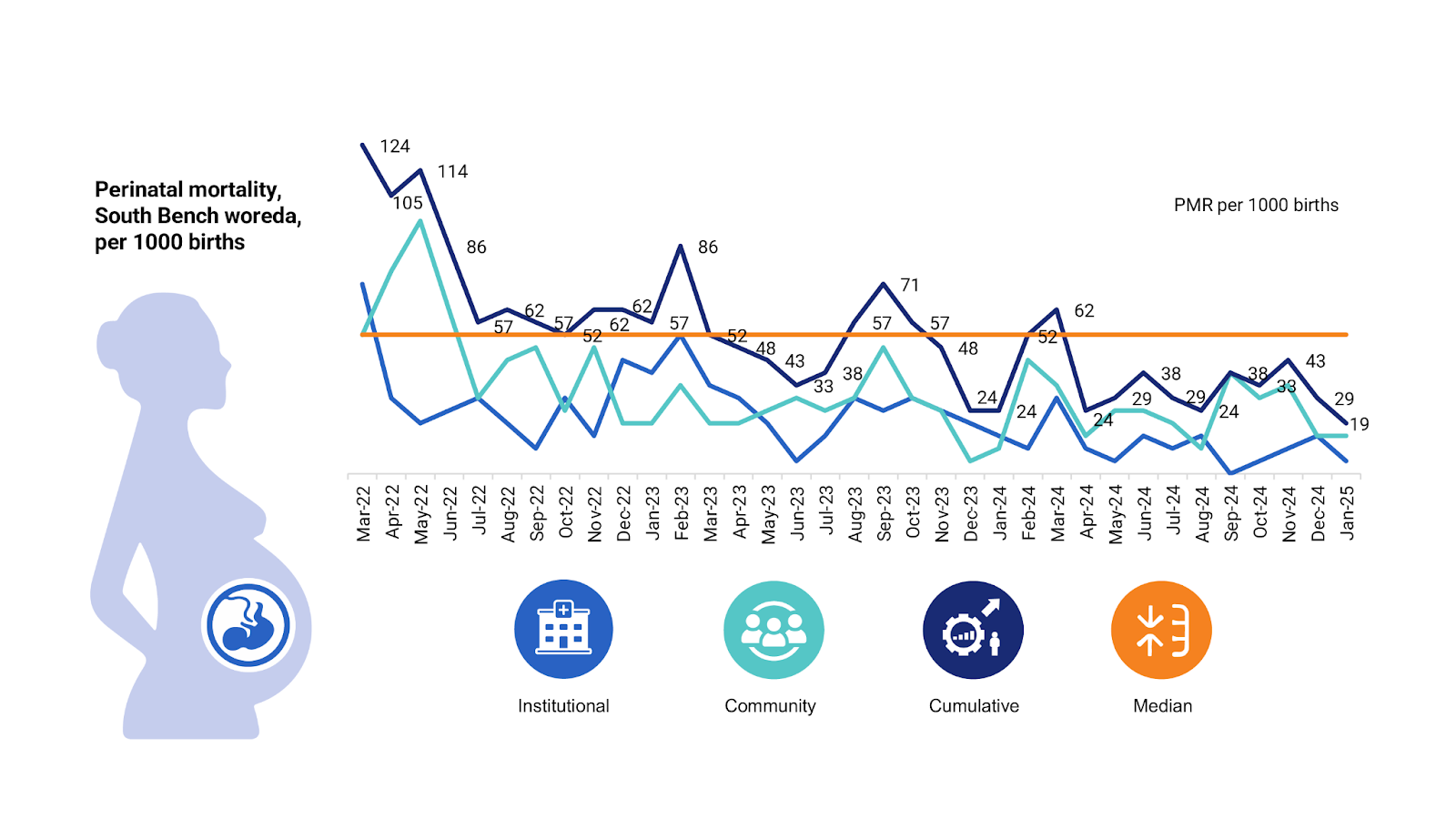
A run chart depicting the change in perinatal mortality rate based on delivery location at South Bench woreda, March 2022–January 2025
A 48% reduction in perinatal mortality is more than a data point; it’s a profound demonstration of what’s possible when communities take ownership of their health. The CCFQI model proves that forging powerful, sustainable partnerships across facilities, communities, and local government is a replicable roadmap for transformation.
We strive to build lasting relationships to produce better health and education outcomes for all.
